top of page

Part 3: The views
Now that we have the set up out of the way, it's time to discuss the next set of concepts when it comes to ECG's.
The questions to be answered are we follows:
Why do we need so many leads?
What are territories?
Why is an escaped pidgeon within the ward the job of the medical registrar to deal with?
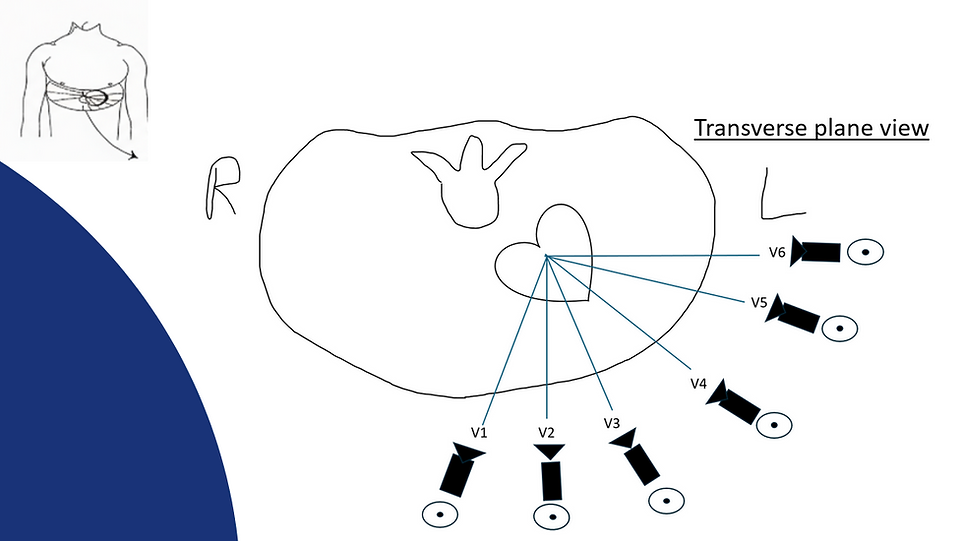
The author again indulges in his inner Picasso and creates this image to demonstrate one of his key concepts.
Each lead only sees the heart from it's perspective.
Each lead can only "see" the waveform as either going towards it, or away from it.
Each lead can thus only interpret this as being either positive or negative, relative to itself.

If we revisit this well-flogged example, the concept of "positive" and "negative" are with respect to whether the waveform is above the line, or beneath it.
This (should) be self-explanatory.
A predominantly "positive" waveform implies the dominant direction of that wave is towards that lead.
The reverse is true.
A predominantly "negative" waveform, implies the dominant direction of that wave is away from that lead.
As such, you will hopefully agree that in lead "aVR" the waveform is negative.
that is because from the view of that lead, the waveform is heading away from it.
This is as opposed to leads such as II, III, aVF - where the waveform is positive, implying that the waveform is heading towards it.

If we recall that the normal progression of a heartbeat is from the sinoatrial node in the (shock horror) atrium, and the end result of this is that it reaches the bottom of the ventricles...
...This can be summarised as the black arrow above.
This (hopefully) demonstrates how each lead reacts when it sees the electrical impulse, and how this affects the resultant complex.

The author relies upon the above image a lot in his lectures.
It is at this point that the limitations of the ECG are apparent, and why interpreting ECG's on isolated leads is a fools errand.
Because a single lead can only tell you what it alone "sees" in absolute -ve or +ve terms, along it's axis alone.
Leads are therefore grouped into territories.
To get more information, we observe what happens across a spectrum of views.

And so the concept of "territories" are born.
This term simply revolves around the fact that certain clusters of leads are well suited, by design or otherwise, to "look" at certain parts of the heart.
In the above example, the predominant problem is that there is ST-E in leads II, III, aVF.

This (poorly) put together slide should summarise/demonstrate this as well.
We therefore arrive at the following:
Inferior: II, III, aVF.
Lateral: I, aVL, V5, V6
Anterior: V1, V2, V3, V4.


This summary slide of views relative to the heart should therefore allow the candidate to appreciate why the territories are grouped as they are.
This is what the author coins as the "cinematic approach".
Each electrical impulse from the heart must be the same one on all leads by definition.***

This basic concept is often lost when things get complicated, yet can be relied upon as being a fundamental truth.

Applying this to the above, the question of whether these are narrow or broad complexes in the anterior leads is then easy.
We know that each "beat" is the same.
Therefore, we simply refer to the other leads.
And as a result, we know these are all narrow complexes.
After this section, you will hopefully understand and thus be able to answer the following:
Why do we need so many leads?
What are territories?
This then leaves the important question which some may have simply have skipped over to get to:
Why is dealing with an escaped pigeon within the ward the job of the medical registrar?
To answer this final query, we ask ourselves:
Does the pigeon need surgery?
Does the pigeon need sedation or intubation?
Is the pigeon pregnant?
The answer to all of these is a resounding:
"No. "
Therefore, the surgical specialities and ITU aren't going to be useful here.
One may ponder "Why can't ED deal with this?" - but the person who ponders this fails to recognise that the pigeon is on the ward.
A patient does not go back to ED from the ward. Direction of traffic is in one direction only.
Therefore, this falls under the remit of the legend that is the medical registrar.
Next up: Axis
Click me for part 4!

***
(Be careful about which beat is synchronised to which - some machines are setup as in this example ECG whereas the limb + praecordial leads are synced to each other, whereas on others they are synced to the long strip)
bottom of page