top of page

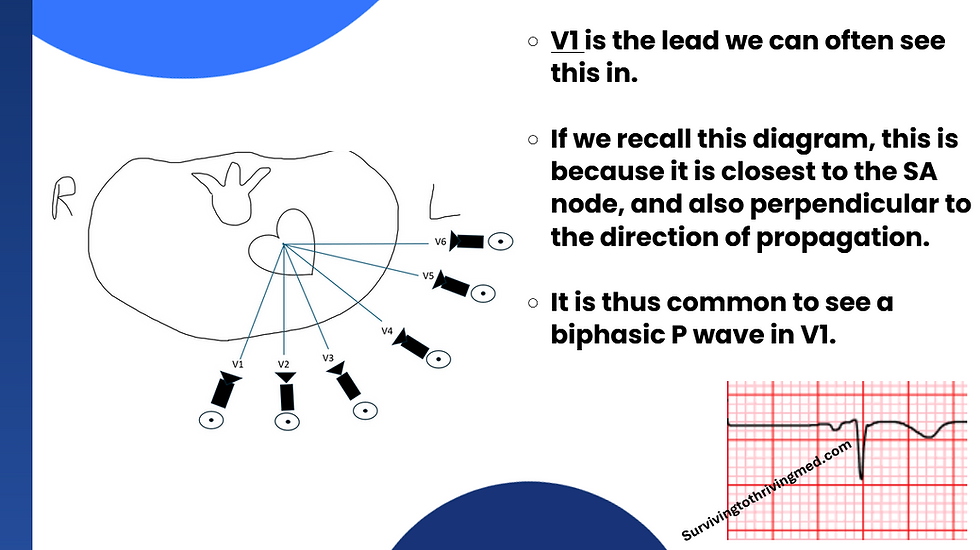
Part 6: The P wave
Every story has a beginning.
Some stories, like Game of Thrones, may have been better off without an end.
Nevertheless, the beginning of our story will actually start at the end.

That is to say, that the paradigm of "PQRST(U)" +/- Delta, Epsilon, Osborn exist within the context of normality.
The first step in interpreting the variant components of an ECG are to understand the following rhythms:




That is because these rhythms are generally considered bad for your immediate health, and you have a high probability of not having a pulse.
Therefore, if you come across one of these in the wild, instead of nerding out over what the ECG shows, you require immediate action.
Like summoning the medical registrar.
On the other hand, if you understand the above rhythms, congratulations - you're pretty much ready to tackle the cardiology section of ALS.
The author will at this point state that the "Advanced" in "ALS" is both subjective and relative to what else exists, and is not an objective measurement.
The author is fairly certain that readers will probably understand that anything without an objective definition will be difficult to quantify, as he has seen "ALS" stand for "Anxiety Level: Severe" as well as "All Logic Suspended" in equal measure.

Back to our original subject matter:
The P wave

This wave depicts the electrical capture when the atrial muscle cells depolarise.
It is worth remembering that due to the following facts:
1) The SA node sits in the R atrium
and
2) The R + L Atrium contract sequentially, rather than simultaneously.
For the anatomically/pathologist orientated, this is via an entity known as the Bachmann Bundle. For people offended by anatomical entities being named after people, alternative titles such as "interatrial bundle" are also used.
Because of this sequential nature of activation, this is sometimes able to be detected upon our beloved ECG.
Indeed, If one remembers our views approach to the ECG, and also recalls how the wave propogates on an axis that is roughly equivalent to an arrow from aVR to II:

This explains why we expect the P wave to be inverted in aVR.
As for which other leads we will tolerate an inverted P wave, that depends upon the source material you read.
The author again reminds the reader that he is a simple ED Doctor and not a cardiologist, and thus has no strong feelings on the matter.
He will, however, invite the reader to observe the following ECG, and how the P waves are misbehaving:

Using our views/vectors approach - we can thus interpret the P waves are now going in the wrong direction, and away from lead II.
Note also, how the QRS axis remains the same.
This is thus an ectopic atrial rhythm - the impulse is transmitted normally via the ventricles, but because of it's location, the leads reveal its sneaky origin.
Some people like absolute definitions, so here are the hard and fast rules:
Normal duration: 0.12s
Amplitude: <2.5mm in limb leads, <1.5mm in praecordial leads

It is an oft quoted myth that the atrial replarisation wave, and thus opposite of the P wave, is buried within the QRS complex.
Observe the following ECG:
This myth is easiest to disprove when the oft expected "hiding spot" for this magical atrial repolarisation wave becomes revealed.
This happens, for example when the QRS decides its terribly bored of being tied to an atrial rhythm, and goes and does its own thing.
The metaphorical QRS mountain has now been moved out of the way, and we can see what goodies were hidden underneath it:
What a disappointment.
Nevertheless, with curiosity now satisfied the reality is that in sacrificing a proper chain of command with respect to coordination of the heart rhythm, the patient has earned themselves a pacemaker.
It is at this juncture that the author will ponder:
Despite wielding a scalpel and installing hardware, the cardiologist is not generally considered a surgeon.
I wonder whose choice this was.
Click for part 7!

bottom of page